The US military set up emergency hospitals in New York City, Los Angeles and Seattle. None of them were ever used for corona virus patients.
The next ridiculous claim being pushed by the Mass Hysteria Media is that we need draconian social distancing in order to “flatten the curve” so that our health care system does not get overwhelmed. Below is an image from April 10, 2020. Fear over Seattle hospitals being overwhelmed with corona virus cases prompted the US military to build a massive field hospital with 250 beds inside of a convention center just south of Seattle. Here is an image of this hospital:
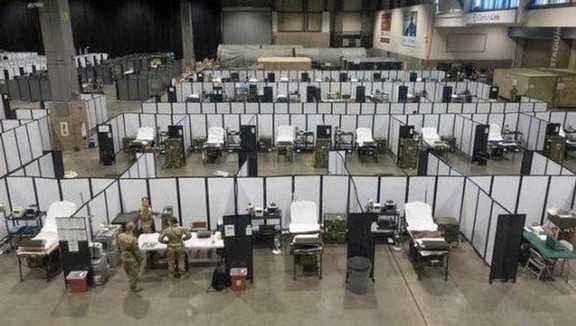
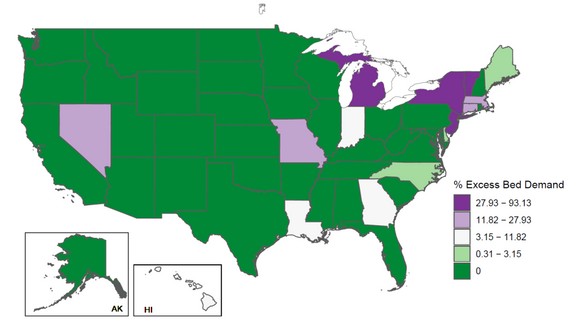
This empty hospital closed after three days without seeing a single patient. The reason it closed was because new cases in Seattle peaked more than a week ago. As I predicted, way back in mid-March, nearly one month ago, local hospitals had no problem handling corona virus cases. In fact, we now know that only 7% of excess beds in hospitals were even used! - 93% empty!
Here is an image of hospital admissions throughout the US in 2020:
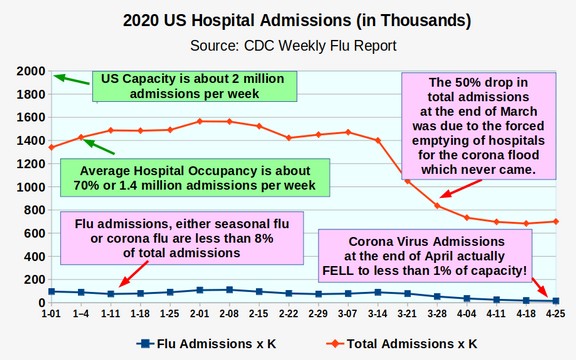
The reason hospital admissions are so important is because they are the most trustworthy and unbiased numbers. The number of Corona Virus “confirmed cases” is simply related to the number of people tested each day. The more people tested, the higher the number gets. Even the number of fatalities is not accurate because we know that hospitals and doctors are strong armed into calling all fatalities corona fatalities. But hospital admissions fly under the radar screen because they are simply a record of how many people check into the hospitals in the US each week – and whether they have flu symptoms. The above chart is therefore one of the most important charts in this entire book, so it is worth looking at it closely.
“Total admissions in thousands” are the red line and “Flu admissions in thousands” are the blue line. The maximum capacity of US hospitals is about 2 million per week. The average number of admissions is about 1.4 million per week (70% of maximum capacity).
Flu admissions, even during winter epidemics, does not exceed 8% of capacity. This is still about 160,000 cases per week. Over a 20 week flu season, this still can be 3 million people – and that is just the people who get such a bad case of the flu, they need to go to the hospital. There are 60 to 100 million other people in the US who get the flu and just stay home and suffer.
Notice that at the end of March, total admissions (the red line) fell 50% - from 1.4 million down to 700,000 admissions per week. This could be the biggest drop in hospital admissions in US history. This huge drop in weekly admissions was due to Stay Home orders around the US that forced hospitals to cancel elective surgeries – even though there was never any chance that the corona virus epidemic would max out capacity. In fact, the corona virus epidemic never even reached the admission rate of the seasonal flu viruses that happened weeks earlier.
The sudden 50% drop in hospital admissions was why hospitals were forced to layoff 50% of the doctors and nurses. The hospital crisis has not been being overwhelmed by the corona virus – but being far below capacity.
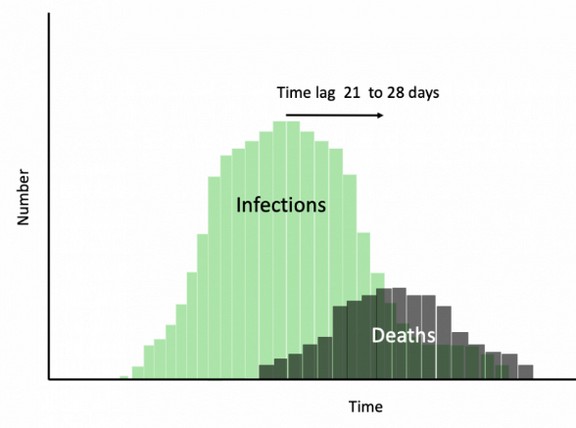
On April 8, 2020, Governor Inslee issued a Press Release attempting to explain why the million dollar military hospital was being dismantled just days after it was built. Instead of stating the obvious – that he had made a huge mistake by greatly over-estimating the risk of the corona virus – he claimed that the reason the giant emergency hospital was no longer needed was because of the success of his social isolation experiment! The reason his claim was ridiculous is because his order had only started 18 days earlier. Even if his order had any effect, it would have taken 10 to 20 days from the time social isolation infections dropped before this drop would be seen in hospital admissions. The truth was the military hospital was never needed.
Inslee also announced that he had returned 400 ventilators that had been given to Washington state by the federal government as these were no longer needed either.
Washington State Department of Health Hospitalization Report
On April 21, 2020, the Washington State Department of Health published a report on hospitalization cases for the corona virus in Washington state. Here is the link to this report: https://www.doh.wa.gov/Portals/1/Documents/1600/coronavirus/covid-hospital-summary.pdf
This report confirmed that Washington State daily admissions never exceeded 80 people and that even this maximum rate occurred in early April and quickly fell back down to less than 40. It is currently less than 10 admissions per day for the entire state and yet the Governor is still keeping the state in a near total business lock down and continues to keep every school and college in the state closed.
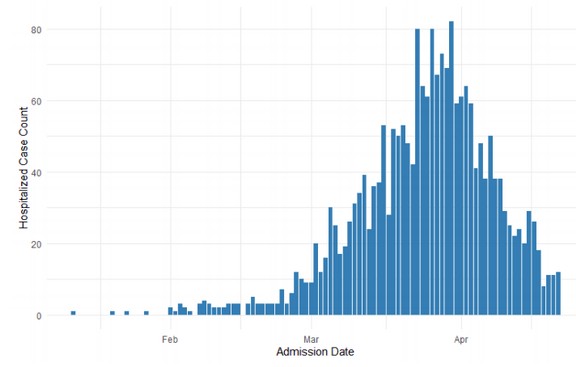
Given that the average hospital stay for flu pneumonia is about 6 days, this places a maximum load on all hospitals in Washington state of only 480 people – and a current load of only 60 people. https://www.wxyz.com/news/coronavirus/henry-ford-health-853-covid-19-patients-discharged-in-last-30-days
This equates to a national maximum load on all hospitals in the US (outside of NYC) of only 24,000 people. Below is an analysis showing that there was never any risk that hospitals in the US or in Washington state were in any danger of being overwhelmed.
Problems with the Claim that US Hospitals will be Overwhelmed
The first problem with this claim is that extreme social distancing did not flatten the curve in the Spanish Flu pandemic in 1918. It simply extended the curve by a couple of weeks. The second problem with this scare tactic of hospitals being overwhelmed is that it does not take into account the actual number of hospital beds and Intensive Care Units and Respirators and Ventilators in the US health care system. We will now take a look at these numbers to see how ridiculous this claim - that corona virus is about to over-run our health care system – really is. Let’s start with the total hospital beds before we consider the Intensive Care Units.
What is the number of hospital beds in the US?
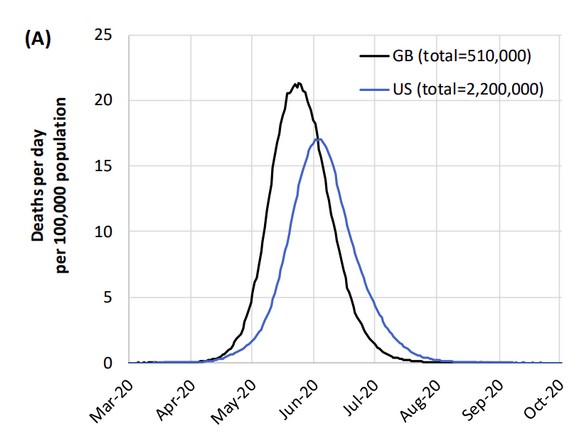
Many fear spreaders in the media like to scare people with the fact that there are only 1,000,000 total beds in American Hospitals despite the fact that we have 330 million people. They point out that there is only one hospital bed for every 330 people. They claim that if the corona virus keeps rising at the current rate, soon all one million hospital beds in America will be full. This might be true if the Ferguson claim of 2.2 million fatalities was accurate. But we have already shown that fatalities in the US could be as low as 99,000. Assume an average mortality rate of 0.1 percent of all cases, this would mean 100 million total cases, I estimate that 0.2% of these cases might require hospitalization (200,000) and that half of these might require Intensive Care Units with Respirators (100,000). These cases will be spread out over a period of at least one month.
But let’s assume for the sake of insanity that all of them showed up at the hospital on the same day. Would such an extreme outcome overwhelm US hospitals? To evaluate this claim, we first need to ask ourselves these important questions:
#1 What percent of corona virus victims require hospitalization? About 20% of diagnosed corona virus cases currently require hospitalization. However, this is because only folks with severe symptoms go to the hospital to get tested and then 20% of these stay in the hospital. As the tests become more widely available, it is likely that the percent that require hospitalization will drop below 1% and may eventually be much less than 1% of actual cases.
#2 How many people are in hospitals with the Corona Virus?
As of April 28, 2020, according to the CDC, there are currently about 1,000,000 cases in the US. https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html
10% of 1,000,000 cases is about 100,000 people in US hospitals. However, the illness only lasts 1 to 2 weeks. So to get the current population, we need to divide the above number by 4 – meaning that less than 25,000 people per week are in US hospitals with the Corona virus. This comes to about 500 people per State. (this was confirmed by the April 21, 2020 Washington State report).
#3 What percent of US hospital beds are being used every day?
The shocking part is that 65% of hospital beds are being used on any given day. So while there are about one million beds, only 350,000 hospital beds are empty. The peak rate of 25,000 people was only 7% of the available hospital beds in the US. Currently less than 1 percent of available hospital beds are being used for corona virus patients!
#4 What about the shortage of respirators and ventilators?
The Mass Hysteria Media has claimed that the real problem is a lack of ventilators. This ignores the fact that even of the people hospitalized, only a fraction need a ventilator. Nevertheless, the US leads the world in ventilators at about 100,000. Even assuming that half of these are already being used, there are still 50,000 unused ventilators. It is unlikely that we will need more than 12,000 – even if everyone needing a respirator showed up on the same day! The real maximum number needed is about 5,000 - which is only 5% of the total number of respirators in the US. I am hoping by now you are starting to see how ridiculous all of the claims being made by the Mass Hysteria Media really are.
The situation is a little tighter in King County and Snohomish County Washington where there are about 6000 confirmed cases in the two counties (the highest concentration in the nation outside of NYC). https://www.doh.wa.gov/Emergencies/Coronavirus
King and Snohomish counties offer about 5,000 staffed hospital beds, of which about 1000 are used for critical care. The median hospital in King and Snohomish counties operated at 50% of its licensed capacity. So there are about 2500 hospital beds and 500 Intensive Care Units available (nearly all of which come with respirators) in King and Snohomish counties. https://www.seattletimes.com/seattle-news/health/short-staffed-and-undersupplied-coronavirus-crisis-strains-seattle-areas-capacity-to-deliver-care/
Divide 5000 total cases by 2 and you get 2500 current cases. 20% of these current cases means that 500 people may be in local hospitals and 100 might need respirators in an Intensive Care Unit. In short, less than 20% of the local hospital capacity is being used even at the peak of the epidemic. https://www.wsha.org/for-patients/coronavirus/coronavirus-tracker/
Most of the current cases are at Evergreen Hospital which is in Kirkland just a few miles from the nursing home with all the fatalities. The age of these patients is 80 to 95 years old – all of which have serious previously existing conditions. Evergreen did reach its capacity recently requiring one patient to be taken to Harborview Medical Center – which is one of many hospitals in Seattle.
Despite the fact that local hospitals have plenty of capacity, the federal government has sent Washington state tens of thousands of respirators, gowns, gloves and other protective gear for health care providers. And just in case the tens of thousands of new respirators are not enough, it turns out that the US military has an entire stockpile of 2,000 more ventilators (some reports say up to 20,000 ventilators!
Ventilators Were Actually Killing Some Patients!
We have already provided links to doctors complaining ventilators were actually killing their patients. On April 8, 2020, AP posted an article called “Some doctors moving away from ventilators for virus patents.” https://apnews.com/8ccd325c2be9bf454c2128dcb7bd616d
Here is a quote: “Some hospitals have reported unusually high death rates for corona virus patients on ventilators, and some doctors worry that the machines could be harming certain patients. 40% to 50% of patients with severe respiratory distress die while on ventilators. But 80% or more of corona virus patients placed on the machines in New York City have died. Some health professionals have wondered whether ventilators might actually make matters worse in certain patients. Experts do say ventilators can be damaging to a patient over time, as high-pressure oxygen is forced into the tiny air sacs in a patient’s lungs.”
“Dr. Eddy Fan, an expert on respiratory treatment at Toronto General Hospital stated: “One of the most important findings in the last few decades is that medical ventilation can worsen lung injury — so we have to be careful how we use it.”
The Washington State Hospital Association has posted this request on their website: “The public should understand that most cases of COVID-19 will not mean hospitalization, or even a trip to an emergency room..”
So if you have serious symptoms such as a shortness of breath, then go quickly to the nearest hospital. But if you just have a fever or the common cold, then stay home, wash your hands and drink plenty of liquids. You should be feeling better in just a few days.
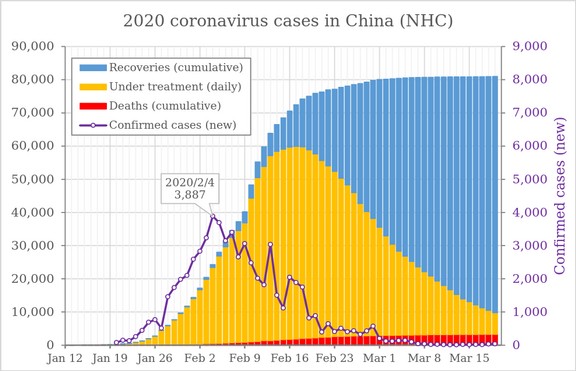
What about the shortage of hospital beds in China?
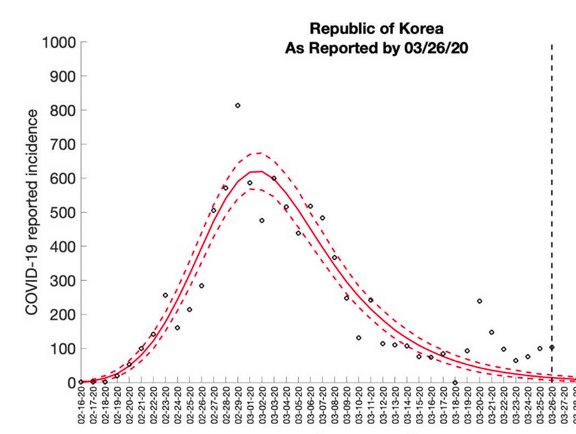
It was reported that the hospital capacity in China was exceeded at the peak of the crisis in China. As we showed in an earlier graph, that peak ran from February 9 to February 23 – a span of nearly two weeks before falling dramatically by the end of February. But even if the peak was exceeded in China, this does not mean the peak will be exceeded in the US. China is a very over-crowded and poor nation compared to the US.
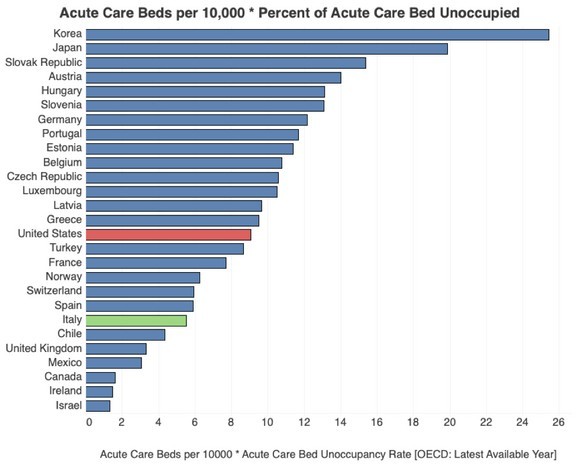
China has so few acute care beds that the rate for China is less than 1 bed per 10,000 people. Put another way, the US has ten times the number of Acute Care beds per 10,000 as does China. So since King County and Snohomish counties has 500 intensive care unit beds, China would have about one tenth this number or 50 intensive care beds. It was the fact that China cannot afford hospitals and Intensive Care Units that was the real problem.
Here is a graph comparing the number of acute care beds per 10,000 in the US versus the rest of the world.
Also, it is unlikely that the outbreak in King and Snohomish counties will be anywhere near as bad as the outbreak in China – for the simple reason that the area in China with the outbreak has some of the worst air pollution in the world – and air pollution is one of the leading causes of pneumonia and depressed immune systems.
Also the outbreak in China was a densely populated area with a high concentration of poor people. Poverty is another contributing factor to depressed immune systems and pneumonia. Nearly all of the victims in China did not die from the corona virus – they died from Pneumonia with Corona Virus being a contributing factor.
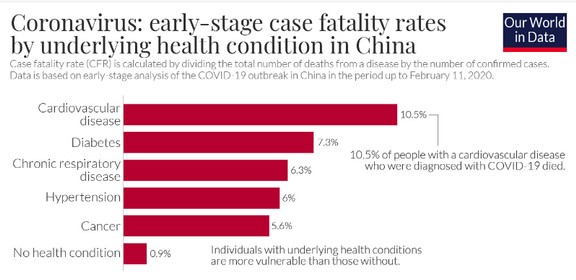
By contrast, King and Snohomish counties have some of the best air conditions in the world. These two counties are among the wealthiest areas in the world – being the world headquarters for Microsoft, Amazon. So it is absurd to be worrying about these two very wealthy counties in Western Washington becoming anything at all like China. Finally, over 99% of the people who died in China had other serious health conditions as is shown by the following chart:
What about the shortage of hospital beds in Italy?
The second place being used to scare people is the corona virus epidemic in Italy. There is a very simple reason that the corona virus is much worse in Italy than in the rest of the world. The clue is that the average age of corona virus fatalities in Italy is over 80. This is because Italy has the second oldest population on earth. Over 20 percent of the population in Italy is over 65 years old. This includes 5 million men and 7 million women for a total of 12 million seniors out of a population of 60 million. In the US, the percent of seniors is only 13 percent. In the UK, it is 16.5 percent.
On March 13, 2020, the President of the Italian National Institute of Health answered questions at a Press Conference in Rome. He stated he had completed a study of the medical records of all of the people who had supposedly died from the corona virus in Italy – and he found only two who did not suffer from other serious pre-existing conditions. Over 99% of victims in Italy suffered from serious pre-existing medical conditions with an average age over 80.
“Corona Positive deceased patients have an average age of over 80 years…The majority of these people are carriers of chronic diseases. Only two people were not presently carriers of [other non-COV] diseases…In fact, authorities are unable to distinguish those who died from the virus, from those who were mostly carriers of other serious diseases and who, therefore, would not have died from Covid-19. “
Another factor that led to a shortage of Intensive Care Unit beds in Italy was the initial lack of available Intensive Care Unit beds. As our previous chart showed, Italy has only half the number of Intensive Care Unit beds per 10,000 population as the US does.
A final factor in Italy which may have over-stated the actual number of corona virus fatalities was the way that cases were being diagnosed. Many of the corona virus fatalities in Italy were never actually tested for the corona virus. Instead they died of pneumonia after they were supposedly exposed to someone with the corona virus and they were assigned a category of “presumptive corona virus.”
Italy has only conducted 42,000 actual corona virus tests — out of a population of 60 million. Thus, less than one person in one thousand has actually been tested in Italy. The US has a much lower percent of very old people and a much higher percent of Intensive Care Units. So once again, it is not accurate to be comparing the situation in the US to the situation in Italy – unless of course your goal is just to scare the hell out of people.
What’s Next?
Now that you better understand the extent to which the media will go to scare us, in the next chapter, we will review why social isolation is not an effective way to stop the corona virus.
{kind=link}